The following provides an example of the overall approach used for the derivation of the machine learning model. Although every effort was made to maintain the overall relationships and trends reflected in real-world data, the approach presented was developed using synthetic data and is used to highlight the thought-process and methodology used for this type of problem. Below is an outline and links to the sample iPython notebooks used for the analysis.
1. Data Profiling
Data Profiling notebook on GitHub: https://github.com/datastudios/healthcare/blob/master/01_Profile.ipynb
The data was made up of three data sources: patient data, patient visit history, and health statistics captured during those visits:
Patient Data
- There are a total of 1,154 patients
- 673 are female and 481 are male
- The minimum age is 23 and maximum age is 103.
- The average age is ~65 years old.
Visit Data
- The date of the visit
- Total visits to date
- Total hospitalizations to date
- Whether the patient was hospitalized during a particular visit (i.e., visit date)
Health Statistics
- Over 170 health statistic data-points were captured including medications taken, blood pressure, and weight among others.
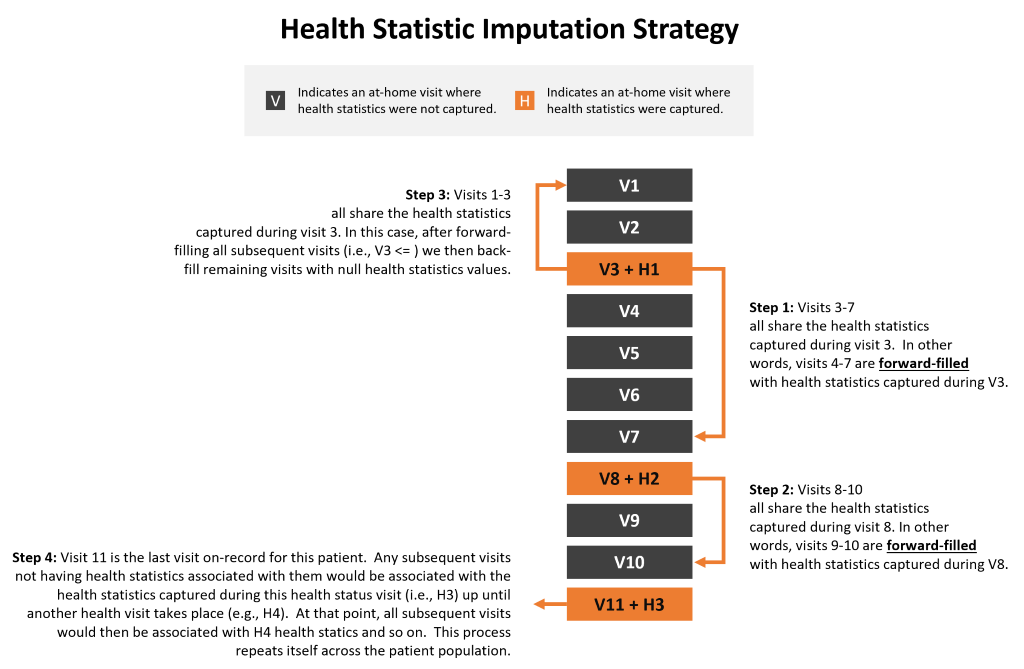
Imputation Strategy
One of the key factors influencing the accuracy of the model's predictions was the imputation strategy for missing data. More specifically, the overall approach for propagating health statistic information captured on some (but not all) at-home health visits would be key. The imputation strategy involved first visits where health statistics were gather and forward-filling those missing values to all subsequent visits up and until there was a more recent set health statistics that had been captured. This ensured that the most recent health data available was associated with visits that came after those statistics were captured. In cases where a visit did not have any health data associated with it after forward-filling, any missing values were then back-filled with the next available health statistic dataset available. And finally, for any patients where a health statistic was never captured (e.g., blood pressure or weight had never been taken) then the mean for the full patient population was imputed. The diagram below provides an overview of this approach:
2. Data Exploration
Data Exploration notebook on GitHub: https://github.com/datastudios/healthcare/blob/master/02_Explore.ipynb
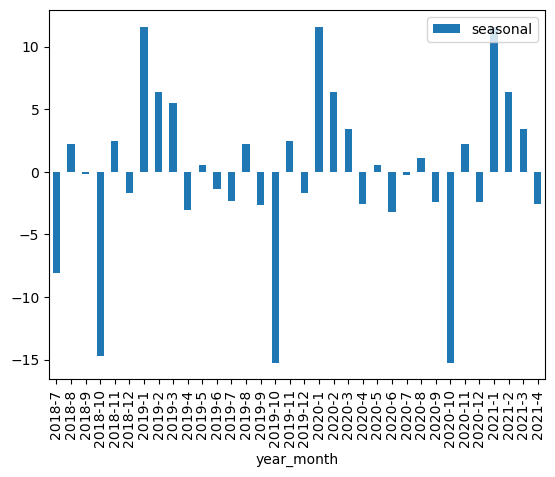
Seasonality
After seasonally decomposing the dataset, it was apparent that their was a clear seasonal component to the data with hospitalizations dropping towards the last quarter of the year and rising sharply at the beginning of each year. This information was used to encode a feature to capture this information.
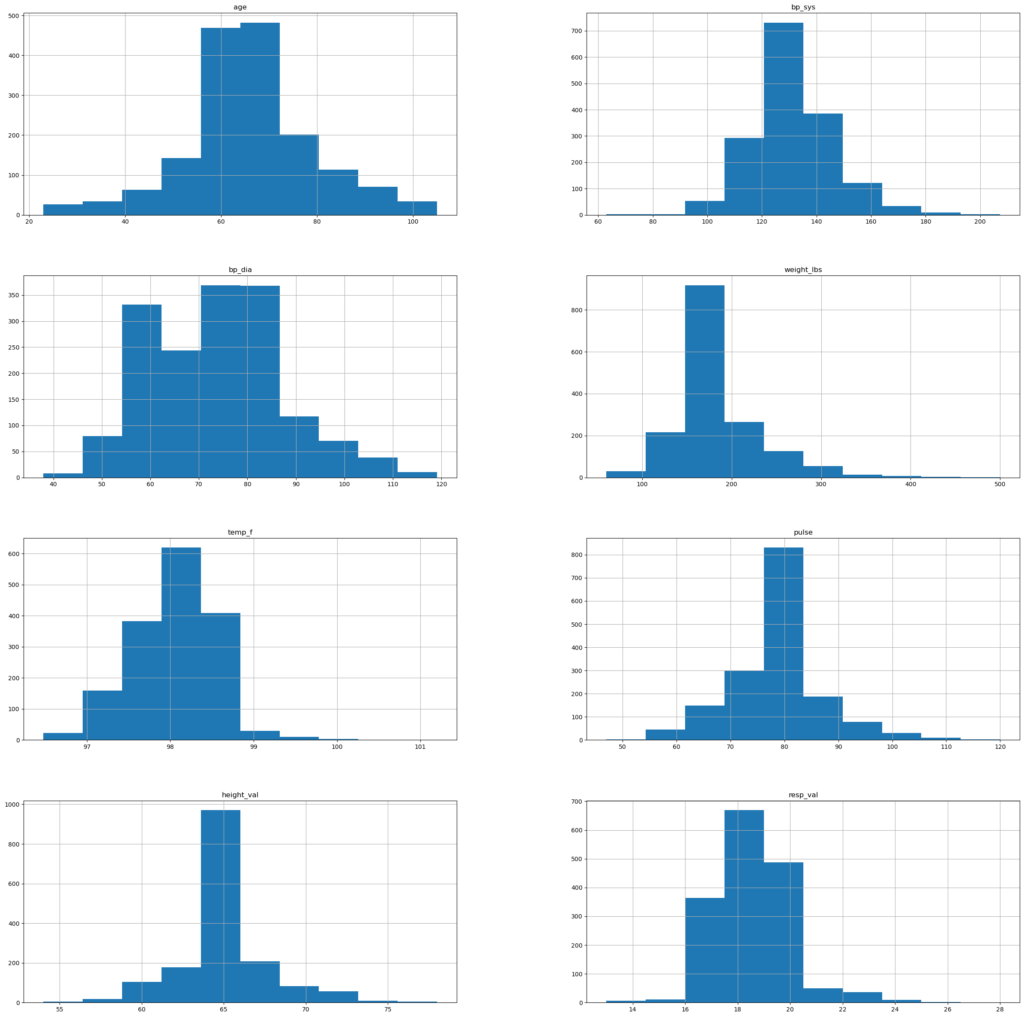
Distribution
The numeric features of the dataset were for the most part symmetrically distributed with the exception of weight. The weight feature was log transformed to address skewness.
Outliers
Outliers were identified based on the numeric features below. There are a few key indicators of health (e.g., blood pressure readings, weight, and age) where outliers on average reflected higher values than non-outliers.
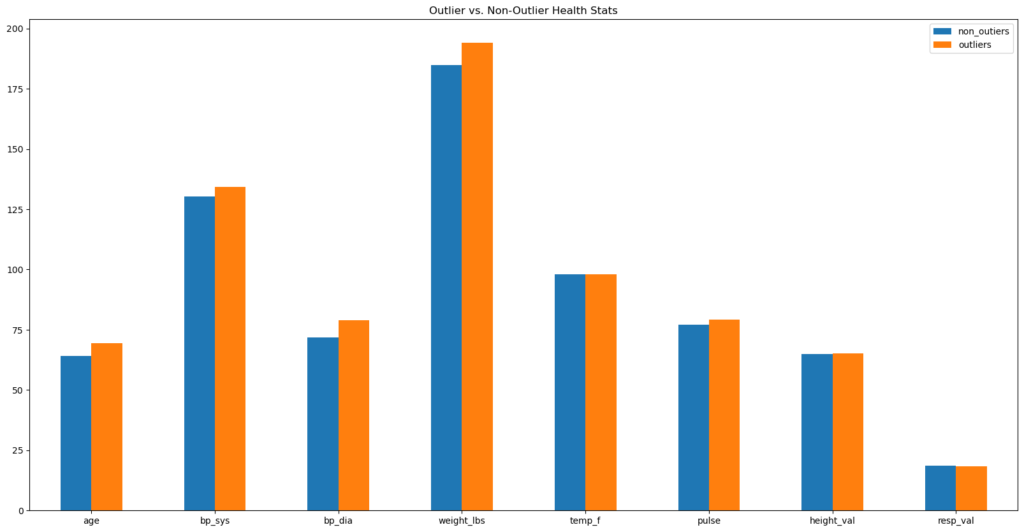
However, it was in the hospitalization per visit ratio that outliers reflected the greatest difference with non-outliers.
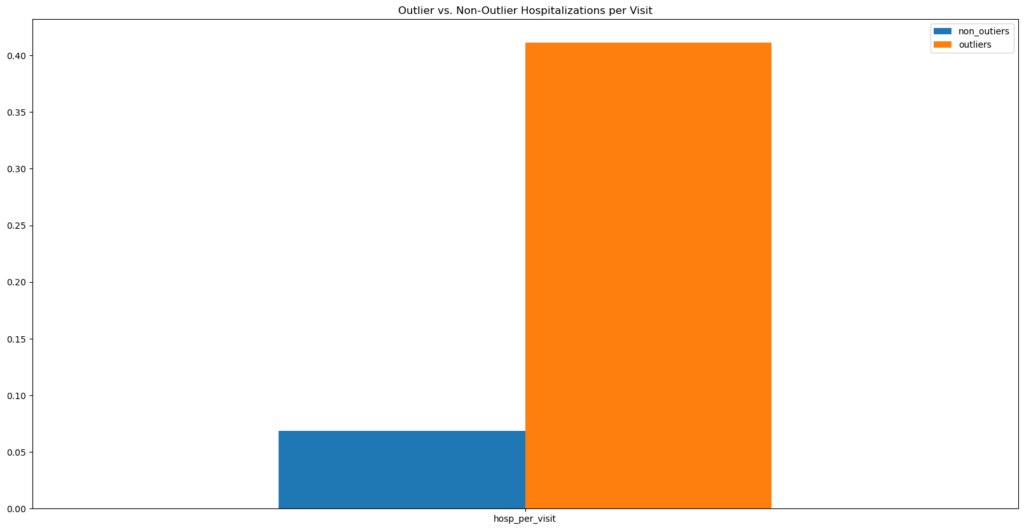
Outliers were not removed from the dataset. However, this information did inform the creation of cluster groups based on the above numeric features to encode this differences.
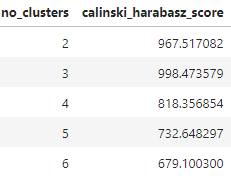
Cluster Creation
There were 3 clusters identified using the Elbow method and Calinski-Harabasz scores.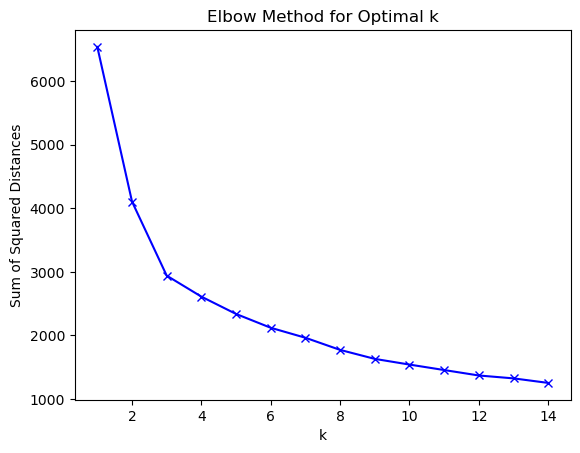
The Calinski Harabasz score confirms 3 clusters being the optimal k.
Lag Variables
Finally, lag variables were created to encode hospitalization and visit history (i.e., hospitalization total, visits total, hospitalization per visit etc.)
3. Prediction
The Prediction and Utilities notebooks bring all the prior profiling and analysis together. The Utilities notebook functions modularize and organizes logic reusable across this and other projects. It also centralizes Scikit-learn custom transformers developed for data transformation and model evaluation steps:
Prediction notebook on GitHub: https://github.com/datastudios/healthcare/blob/master/03_Predict.ipynb
Utilities notebook on GitHub: https://github.com/datastudios/healthcare/blob/master/utils/utils_diagnosis.ipynb
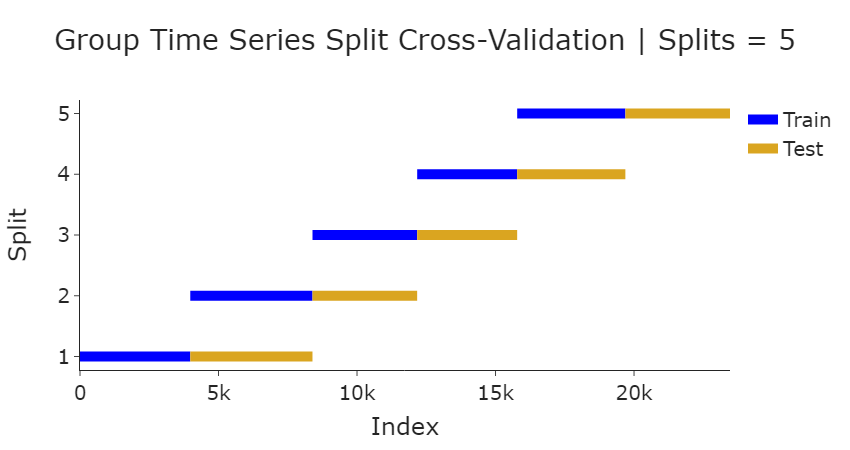
Group Time-Series Cross-Validation
The nature of the dataset requires a time-series based cross-validation approach (a typical random split of the data wouldn't work in this case as it would cause data leakage with future observations "leaking" into training data). Furthermore, the dataset observations may be unevenly grouped since each patient has a different set of visits. So, we'll need to group the train/test splits so that they are split as evenly as possible. The GroupTimeSeries Split API was leveraged as a basis for the custom transformer developed for our pipeline. The diagram below shows the dataset split with the number of splits = 5:
Preprocessor Pipeline
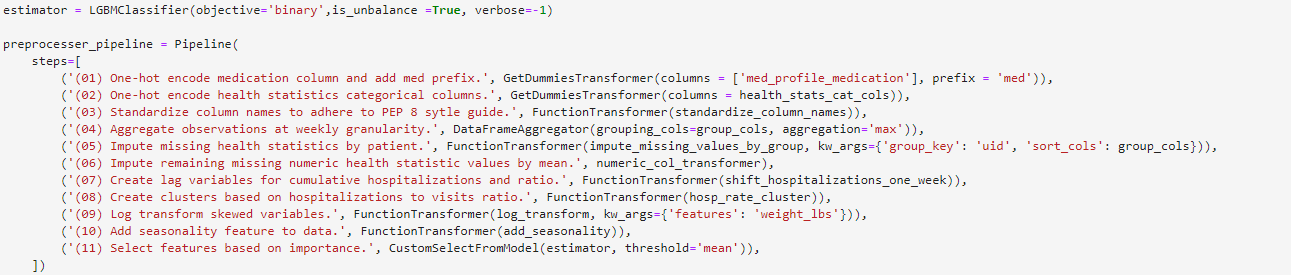
The preprocessor pipeline reflects the functions and custom Scikit-learn classes developed (Step descriptions are purposely verbose, in a production setting these would be kept succinct to allow for experimentation):
Pipeline with Estimator
The full pipeline includes the preprocessing steps along with a custom Scikit-learn RandomizedSearchCV class that instantiates a GroupTimeSeriesSplit object to be used for cross-validation of all models to be tested.

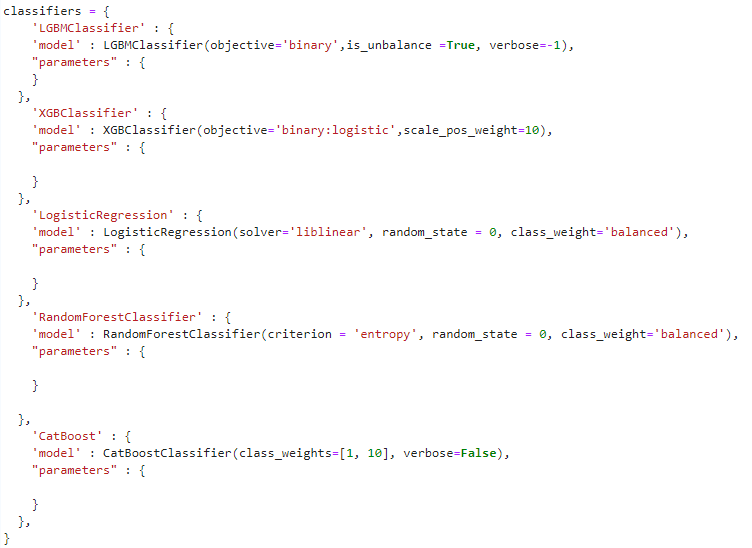
Classifier Dictionary
The classifier dictionary is the data structure containing all models and parameters to be cross-validated. In the example below, we start with baseline parameters. In subsequent steps, we input a distribution of hyperparameters selected for optimization.
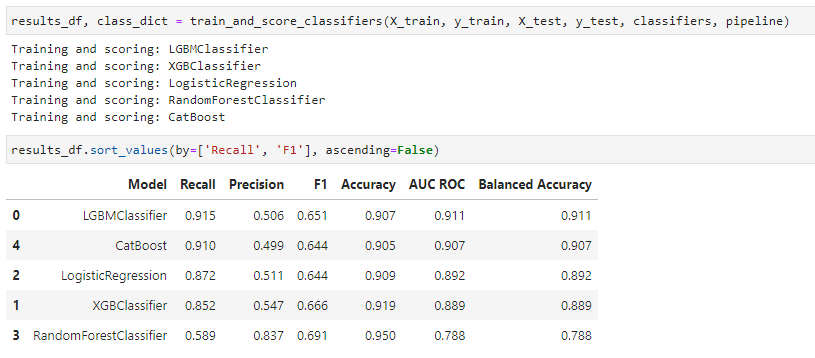
Evaluation Function
The evaluation function trains and tests the various models submitted via the classifiers dictionary instantiated previously based on the pipeline steps defined. It returns a data frame containing a summary of results based on the test data submitted and a dictionary containing fitted models along with their predictions.
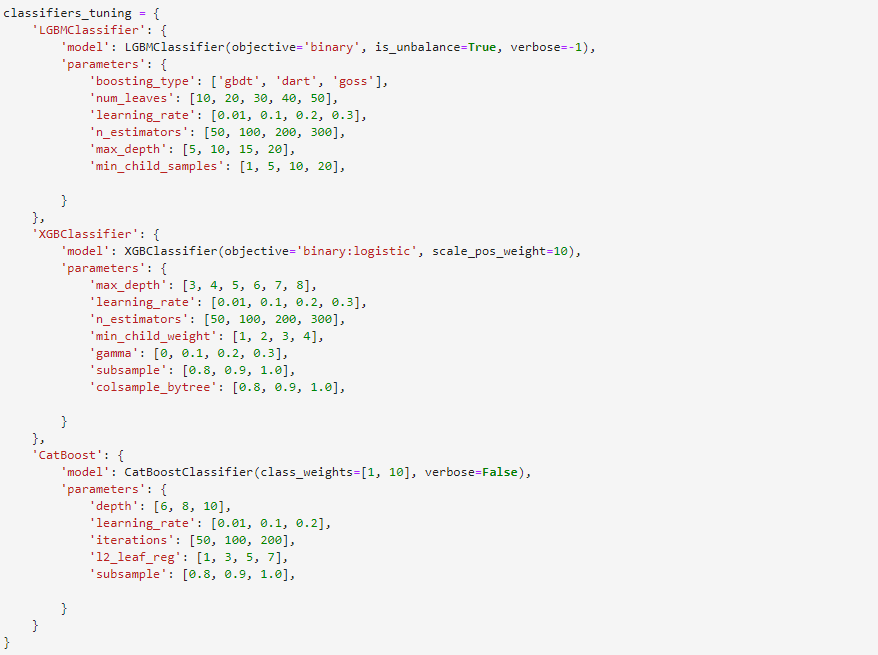
Once the results of the initial set of baseline models is assessed, we can further tune a subset of performant models:
And again obtain result objects as described previously:
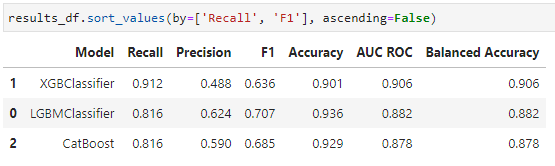
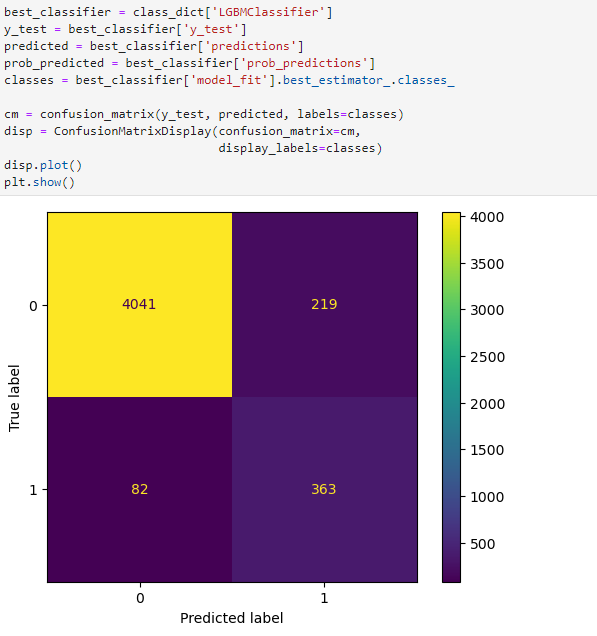
Analyze Results
We can then further analyze the results of a candidate model for production. (Here we only show a confusion matrix, but typically we'd want to use a library such as SHAP to better understand and explain the output of the model)
Write Data for BI Tool
Data was then provided for further analysis by business domain experts via their preferred BI tool. (In this example, to CSV files but data was written to the data warehouse for the production version)

